
Overview of HFEA public consultation on Choose a Fertility Clinic 2025
Consultation held August-September 2025 on clinic’s main profile statistics on the Choose a Fertility Clinic webpage
Published: December 2025
Table of contents
- Introduction
- Main points
- Summary of findings from the consultation
- About the HFEA
Introduction
The HFEA has a statutory duty to provide information to the public about fertility treatment. Using the data collected from licensed fertility clinics, we publish verified information on the outcomes of treatment as well as inspection findings and information about the services a clinic provides via Choose a Fertility Clinic (CaFC) on the HFEA website.
The CaFC data was last reviewed in 2016-17 after consultation and testing. However, since then, the fertility sector has changed significantly (find out more here). Additionally, following the migration of the HFEA’s register data to a new database and the introduction of the new data submission system, PRISM, the CaFC tool has not been updated for some time.
The HFEA Authority discussed CaFC in May 2025 and July 2025. The Authority agreed that a focused consultation should take place over the summer to gather the views of clinic staff and patients on all clinics’ main profile page statistics. The consultation received responses from a range of stakeholders including current, prospective and past patients, members of the public, organisations, and professionals. Around a third (35%, 97) of responses came from individuals sharing their personal views or experiences, either as a patient (31%, 85) or as a member of the public (4%, 12). Just under half (44%, 121) of responses came from professionals and 20% (55) of responses were submitted on behalf of organisations.
We saw some differences in preferences for the way in which outcomes of treatments at a clinic could be presented on a clinic’s main profile page between response groups. Generally, all response groups agreed on what treatments should be included or excluded from a clinic’s main profile page statistic, with some exceptions. There were some detailed responses providing further context to the views shared.
Some respondents provided their views on the ways statistics could be displayed to increase clarity for patients and the public or stated additional information that would add important context. While outside the scope of this consultation, the Authority agreed that following the publication of the full CaFC later in 2025, a review of the different information sources held on the HFEA website should be undertaken. This is planned for during the current strategic period of 2025-2028.
A summary of the consultation findings presented to the Authority is available here. A recording of the meeting is available to view here and papers from the meeting can be found here.
The HFEA would like to thank every individual and organisation who took the time to respond to our consultation. Each response has been read in detail and helped inform the Authority’s decision.
Main points
- A total of 273 responses were included in final analysis.
- Differences between the preferences expressed for the four options were small.
- Most preferred statistic out of the four options presented was births per embryo transferred (3.37), followed by births per egg collection procedure (3.31). The least preferred were births per cycle started and births per embryo transfer procedure (both 3.22).
- Differences in preferences on a clinic’s main profile page statistic were seen between groups.
- Patients and members of the public’s most preferred method was births per cycle started (3.73 and 3.50, respectively). Organisations’ most preferred method was births per egg collection procedure (3.58) and professionals’ was births per embryo transferred (3.68).
- Most respondents (77%) did not think that there should be one combined statistic presented.
- Most respondents (80%) were in favour of including a combination of both fresh and frozen embryo transfer cycles in the main profile page statistic.
- Almost 70% (69%) of respondents were in favour of excluding treatments using donor eggs in a clinic’s main profile page statistic, while 23% were in favour of including treatments using donor eggs. However, differences were seen between response groups.
- Half (51%) of respondents were in favour of excluding treatments using PGT-A from a clinic’s main profile page statistic, but differences were seen across response groups.
| Table 1. Summary of consultation findings overall and per response group | ||||||||
|---|---|---|---|---|---|---|---|---|
| Group | Births per cycle started | Births per egg collection procedure | Births per embryo transfer procedure | Births per embryo transferred | Combined rate | Include fresh & frozen | Include donor eggs | Include PGT-A |
| Overall (N=273) | 3 | 2 | 3 | 1 | × | ✓ | × | × |
| Patients (N=85) | 1 | 4 | 3 | 2 | × | ✓ | × | - |
| Professionals (N=121) | 4 | 2 | 3 | 1 | × | ✓ | × | × |
| Organisations (N=55) | 3 | 1 | 2 | 4 | × | ✓ | × | × |
| Public (N=12) | 1 | 2 | 3 | 3 | × | ✓ | - | × |
| Note: Respondents who answered yes to presenting a clinic’s main profile page statistic as a combined rate were excluded from analysis of questions asking for preferences on the inclusion/exclusion of fresh and frozen embryo cycles and treatments using donor eggs, PGT-A. A response group was deemed as being in favour of including/excluding a treatment when over 50% of the respondents within that group agreed. A “–” has been used to highlight cases where no clear preference was found. Further information on key findings is summarised in Main findings section. | ||||||||
Main findings
Overview of response groups
A total of 273 complete, submitted responses were included in the analysis (Table 2). The methodology for data collection and analysis can be found in the accompanying quality and methodology report.
Just over 35% of responses came from individuals sharing their personal views or experiences, either as a patient (31%) or as a member of the public (4%).
Just under half (44%) of responses were professionals and 20% were submitted on behalf of organisations. See full list of the organisations who responded to consultation.
Most professionals worked at HFEA-licensed clinics (86%). Over half (64%) of those were working at private clinics compared to 27% at NHS clinics. A large proportion of the responses submitted by organisations came from those working at HFEA-licensed clinics (70%). 13% were submitted on behalf of a professional body or organisation and 15% were submitted by a UK group, organisation or charity that represented patients.
| Table 2. Number of responses by group | ||
|---|---|---|
| Response group | Number of responses | Percentage |
| Prospective, current, or past patient | 85 | 31% |
| Interested member of the public | 12 | 4% |
| Individual sharing professional view | 121 | 44% |
| On behalf of an organisation* | 55 | 20% |
| Total | 273 | 100% |
| Q: In what capacity are you responding to this consultation (please select only ONE option) This was a required question. *where possible, organisational responses were validated (N=273). | ||
Download the underlying data for Table 2 as Excel Worksheet
Main profile page statistic: which was the preferred rate?
The consultation presented four different options for displaying a clinic’s main profile page statistic, providing context and a summary of potential benefits and drawbacks with each metric. Respondents were able to rank options in order of preference from one to four (one being most preferred, four being least preferred). They were also able to indicate whether they would not choose an option at all.
Differences between the preferences expressed for the four options were small. However, overall, the consultation found that the most preferred statistic out of the four options presented would be births per embryo transferred (3.37), followed by births per egg collection procedure (3.31, Figure 1). The least preferred metrics were births per cycle started and births per embryo transfer procedure (both 3.22).
When looking at the distribution of responses, some options had mixed views, with preferences at either end of the spectrum. Births per embryo transferred and births per cycle started had the highest proportion of respondents ranking these as their most preferred statistic (33% and 32%, respectively). However, these options also had the highest proportion of respondents ranking them as their least preferred statistic (23% and 26%, respectively). When looking at results per response group, these differences in preferences become more evident.
Preference varied by response group, with patients most preferring births per cycle started (3.73), and births per embryo transferred (3.26, Figure 2). Professionals most preferred births per embryo transferred (3.68), whereas organisations preferred births per egg collection procedure (3.58).
Figure 1. Preference of a clinic’s main profile page statistic
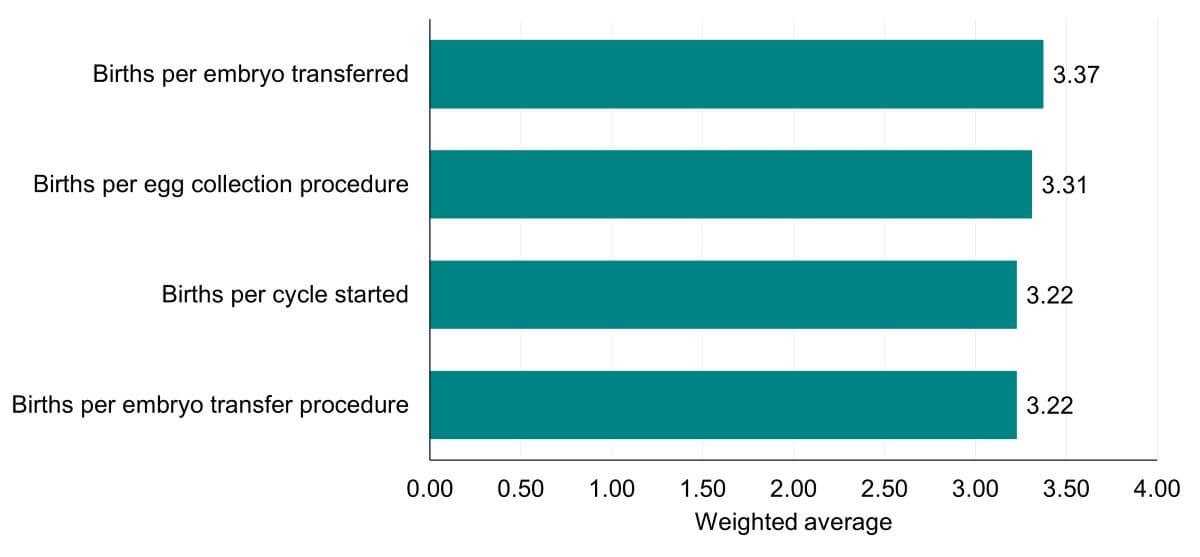
Q: Which of these options do you think should be a clinic’s main profile page statistic? Please place the below options in order of preference from one to four (one being most preferred, four being least preferred option) by either dragging and dropping with your cursor or selecting a number from the box on the left-hand side. This was a required question (N=273).
Download the underlying data for Figure 1 as Excel Worksheet
Figure 2. Preference for presenting a clinic’s main profile page statistic by response group
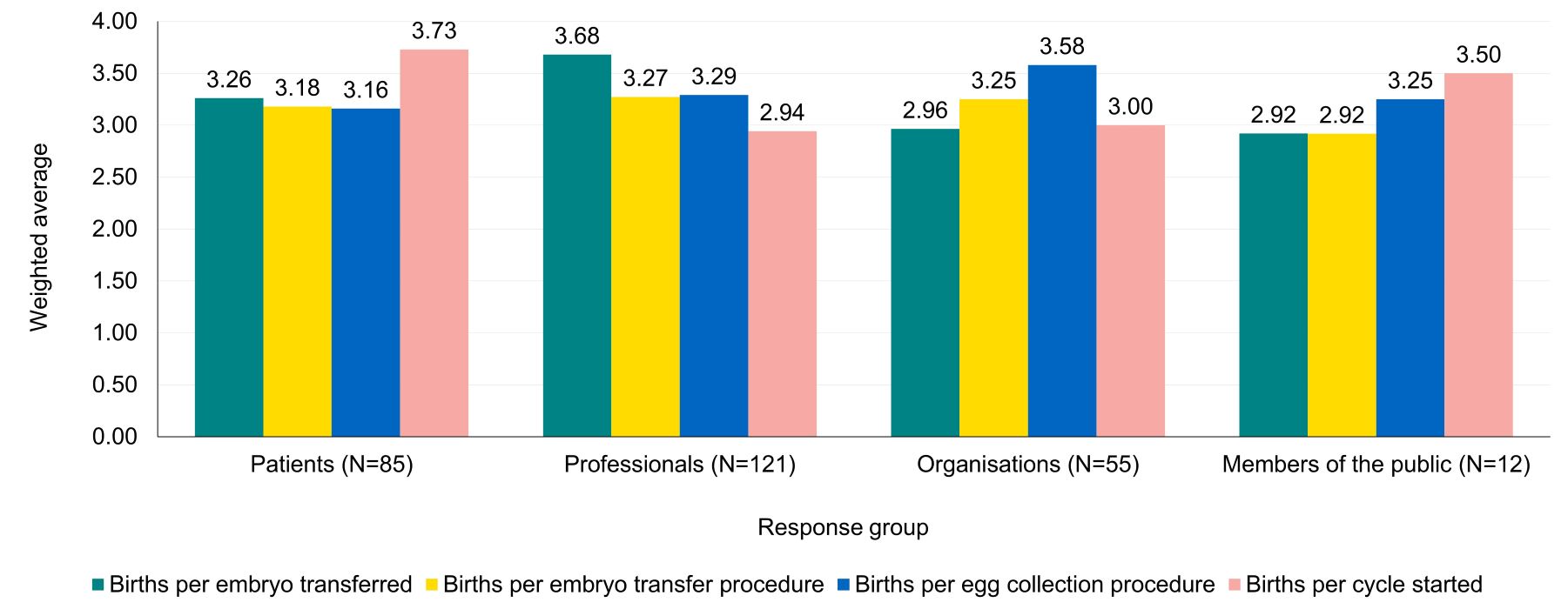
Q: Which of these options do you think should be a clinic’s main profile page statistic? Please place the below options in order of preference from one to four (one being most preferred, four being least preferred option) by either dragging and dropping with your cursor or selecting a number from the box on the left-hand side. This was a required question. (N=273).
Download the underlying data for Figure 2 as Excel Worksheet
Free text responses received from professionals and organisations often provided further context. The quotes provided throughout this report give an indication of some of the views expressed.
Some professional and organisational responses felt births per cycle started would be a suitable profile page statistic as it “accurately reflects the patient journey from the very start of treatment”. Another common reason stated was that it would represent differences in laboratory performance. Others voiced concerns that this may lead to clinics taking on fewer poor prognosis patients or “penalis[ing] patient-friendly strategies such as minimal stimulation, cancelled cycles, or multiple egg collections”.
Births per embryo transferred was preferred by organisations and professionals as it “takes into account the quality of embryos and encourages single embryo transfer”. Some others felt it does not provide a full picture for patients, as it does not include cycles that do not reach embryo transfer stage. Similar views were given about birth per egg collection procedure and births per embryo transfer procedure, although fewer respondents mentioned these statistics.
“There are positives and negatives for each option of how to present the data and if presented in isolation as only one option, then we run the risk of some clinics and patients not being fairly represented. As a clinic we feel that per cycle started is the fairest option…”
-Anonymous, on behalf of an organisation.
A small number of responses from organisations and professionals proposed different ways of presenting a clinic’s main profile page statistic, such as live birth per new patient over a defined period or live births after a euploid (embryos with the correct number of chromosomes) embryo transfer.
Patients commented on being in favour of a statistic showing the portion of cycles resulting in a baby from the start of treatment. They also often referred to additional information they would like to see alongside any statistic.
“What is key to me as a patient is to understand how successful I am likely to be with a specific clinic, so it is key that the option of seeing success per cycle started is included. This is important because birth per embryo transfer or embryo transferred obscures the situations where the treatment doesn't yield any eggs or any viable embryos - from patient's perspective this is just as bad if an outcome as transferring an embryo and not resulting in success”
-A prospective, current or past fertility patient sharing personal views.
Many responses across different groups stressed that regardless of method, there was a need to ensure that statistics were presented in plain language. There were also suggestions to improve understanding and reduce the risk of misinterpretation of methods such as visual aids or text summaries.
“…We also strongly recommend that statistics are presented with clear explanatory notes, plain-language definitions, and reliability ranges, so that patients understand both the meaning and the limitations of the figures. Patients frequently report feeling confused or distressed when interpreting success rates, and additional context helps prevent misinterpretation”
-Organisational response from British Infertility Counselling Association.
“The statistics need to [be] clearly understandable by lay public and also meaningful. It's that we understand what the chances are of having a baby with the treatment type we choose. We don't want to be bamboozled by births per embryo transferred or per cycle etc, we need to know what are our chances of having a successful live birth.”
-A prospective, current or past fertility patient sharing personal views.
Presenting a combined rate
Respondents were asked whether the clinic’s main profile statistic should be presented as a combined statistic. This means the statistic could include all types of IVF, such as fresh and frozen embryo transfers and treatments using donor eggs or PGT-A. Most participants (77%) did not think that there should be one combined statistic (Figure 3).
This was seen across response groups with over 70% of patients, professionals, and organisations in agreement (Figure 4). While a high proportion of public respondents were unsure (25%), most (58%) did not think that the clinic’s main profile statistic should be presented as one combined statistic.
Figure 3. Views on presenting the main profile page statistic as a combined statistic
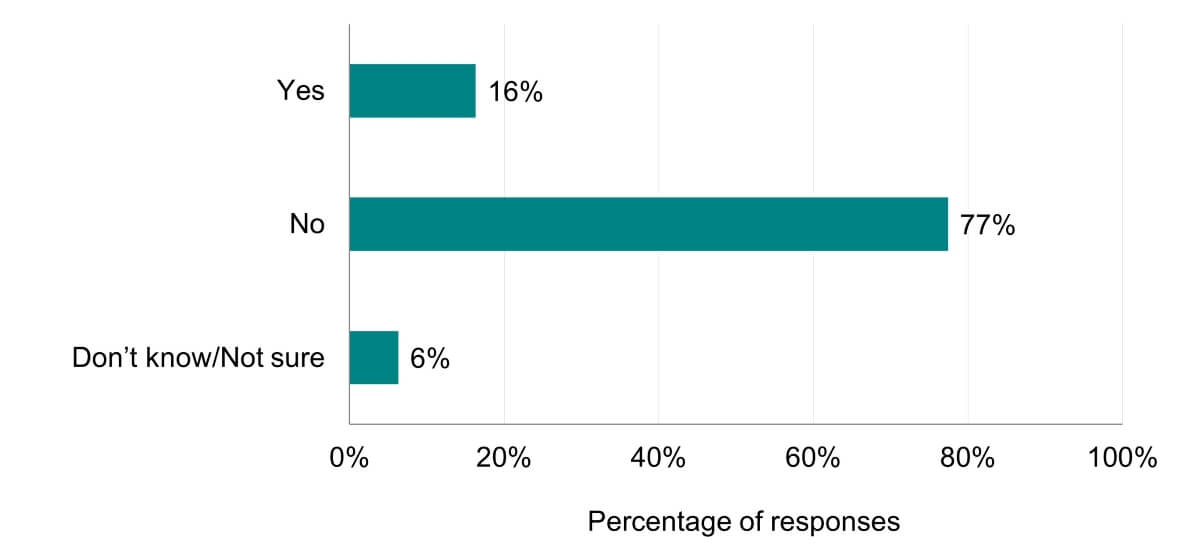
Q: Do you think there should be one combined statistic that includes all different types of IVF treatment (fresh and frozen embryo cycles, donor eggs and PGT-A cycles)? Percentages are calculated on the total number of respondents to the question, rather than total respondents to consultation overall. A total of three respondents skipped this question (N=270).
Download the underlying data for Figure 3 as Excel Worksheet
Figure 4. Views on presenting the main profile page statistic as a combined statistic by response group
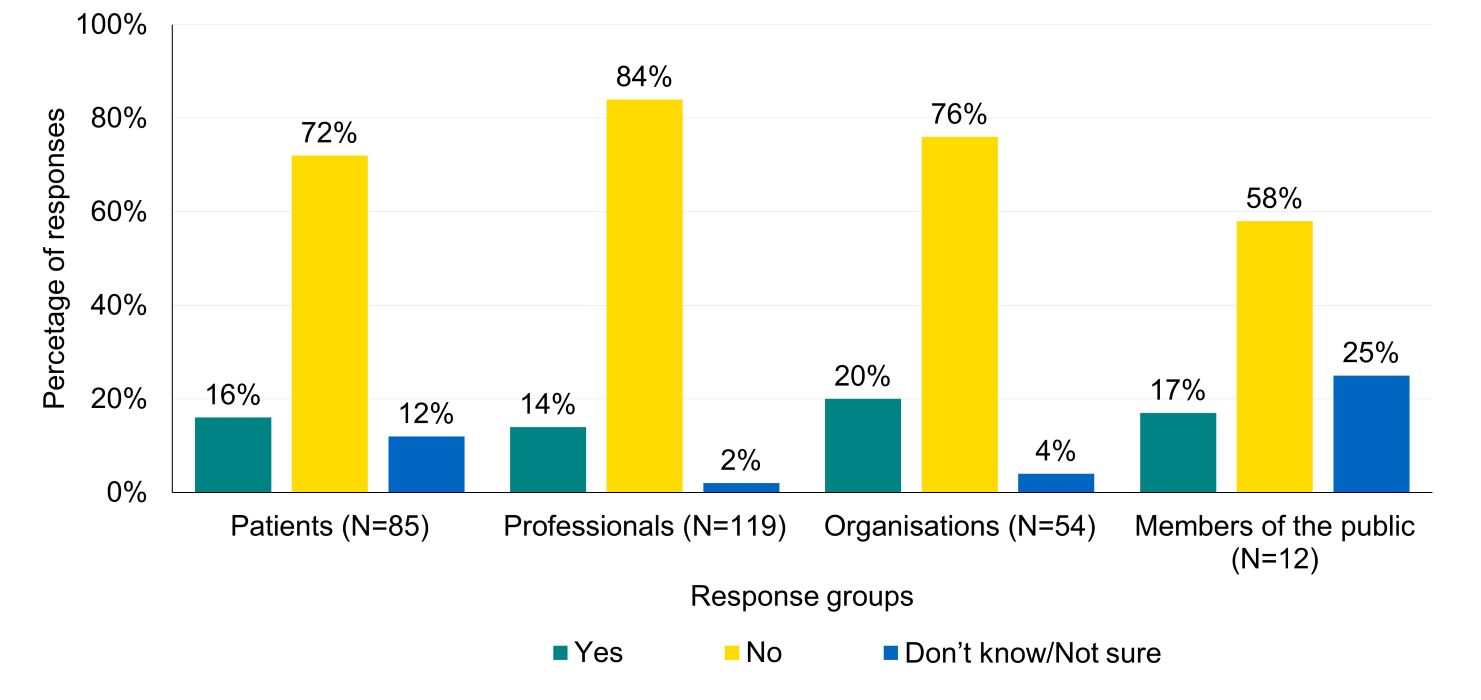
Q: Do you think there should be one combined statistic that includes all different types of IVF treatment (fresh and frozen embryo cycles, donor eggs and PGT-A cycles)? Percentages are calculated on the total number of respondents to the question, rather than total respondents to consultation overall. A total of three respondents skipped this question (N=270).
Download the underlying data for Figure 4 as Excel Worksheet
A common reason from professionals and organisations on why they did not want a combined rate was that it would reduce the “meaning” of the statistics presented as different treatments may be used for different reasons/conditions. The distortion of outcomes was also mentioned particularly for treatments that have the potential to “manipulate” reporting outcomes and lead to a statistic that may mislead patients and the public. One patient echoed this point of view.
Inclusion of different treatment types
Respondents were then asked to indicate their preference for treatments to include in a clinic’s main profile page statistic, if it was not presented as a combined rate. This includes consideration for inclusion of fresh/frozen embryo transfers, treatments using donor eggs, or using PGT-A.
Fresh/frozen embryo transfer
Most respondents (80%) were in favour of including a combination of both fresh and frozen embryo transfer cycles in the main profile page statistic. Only 15% preferred only including fresh embryo transfer cycles (Figure 5).
Over 70% of all response groups preferred for the statistic to include both fresh and frozen embryo transfers (Figure 6).
Figure 5. Views on including fresh and/or frozen embryo cycles in a clinic’s main profile page statistic

Q: Which of the following would be your preference if births per embryo transfer procedure or births per embryo transferred was chosen as a clinic’s main profile page statistic? Percentages are calculated on the total number of respondents to the question, rather than total respondents to consultation overall. Respondents who answered that yes to presenting the profile page statistic as a combined rate were excluded from this question (N=44). A total of three respondents skipped this question (N=223).
Download the underlying data for Figure 5 as Excel Worksheet
Figure 6. Views on including fresh and/or frozen embryo cycles in a clinic’s main profile page statistic by response group
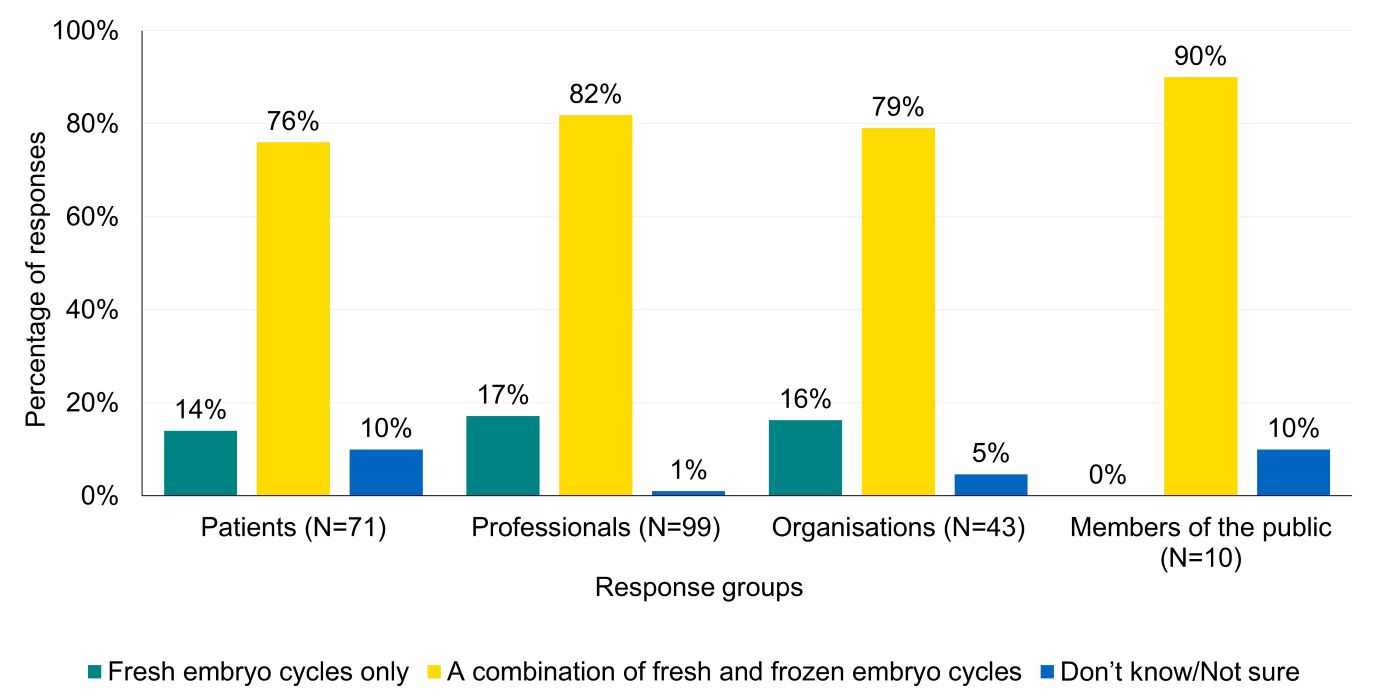
Q: Which of the following would be your preference if births per embryo transfer procedure or births per embryo transferred was chosen as a clinic’s main profile page statistic? Percentages in the above figure are calculated on the total number of respondents to the question, rather than total respondents to consultation overall. Respondents who answered that yes to presenting the profile page statistic as a combined rate were excluded from this question (N=44). A total of three professionals skipped this question (N=223).
Download the underlying data for Figure 6 as Excel Worksheet
Many free text responses from professionals and organisations mentioned whether fresh or frozen embryo cycles should be included. Most preferred for fresh and frozen embryo transfer cycles to be reported on separately, rather than combined. Some suggested providing further context if the rates were combined, such as reporting the ratio of fresh and frozen cycles.
Donor egg treatments
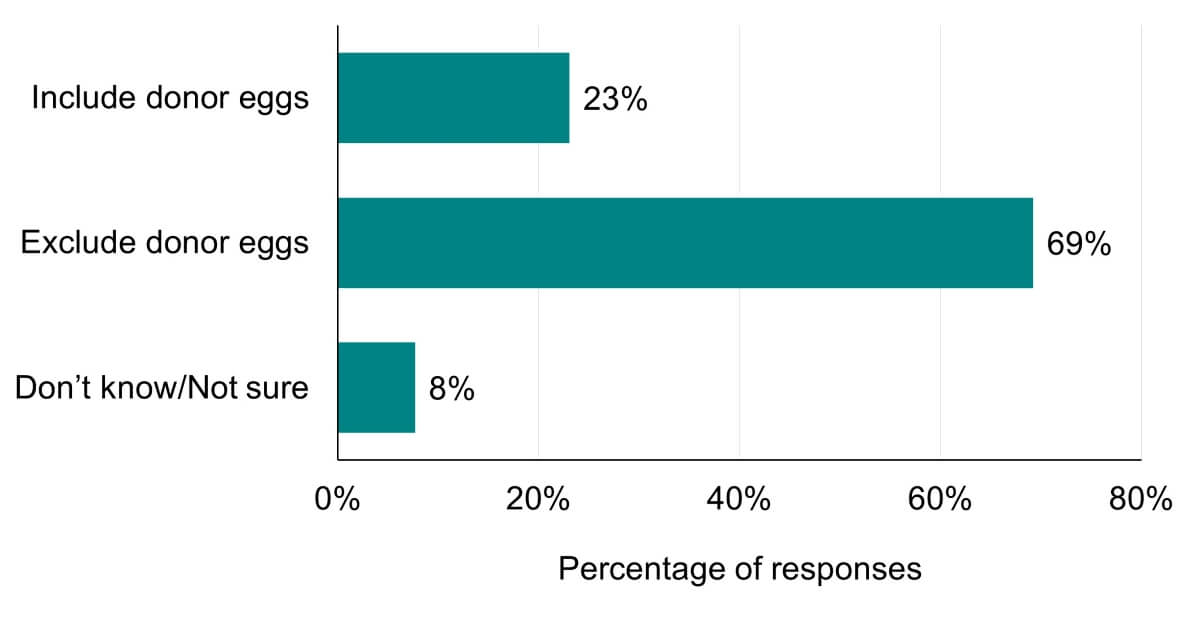
Over 69% of respondents were in favour of excluding treatments using donor eggs in a clinic’s main profile page statistic while 23% were in favour of including (Figure 7). Similarities were seen between most response groups (Figure 8).
Figure 7. Views on including treatments using donor eggs in a clinic’s main profile page statistic
Q: Should treatments using donor eggs be included or excluded from a clinic’s main profile page statistics? Percentages in the above figure are calculated on the total number of respondents to the question, rather than total respondents to consultation overall. Respondents who answered that yes to presenting the profile page statistic as a combined rate were excluded from this question (N=44). A total of five respondents skipped this question (N=221).
Download the underlying data for Figure 7 as Excel Worksheet
Figure 8. Views on including treatments using donor eggs in a clinic’s main profile page statistic by response group
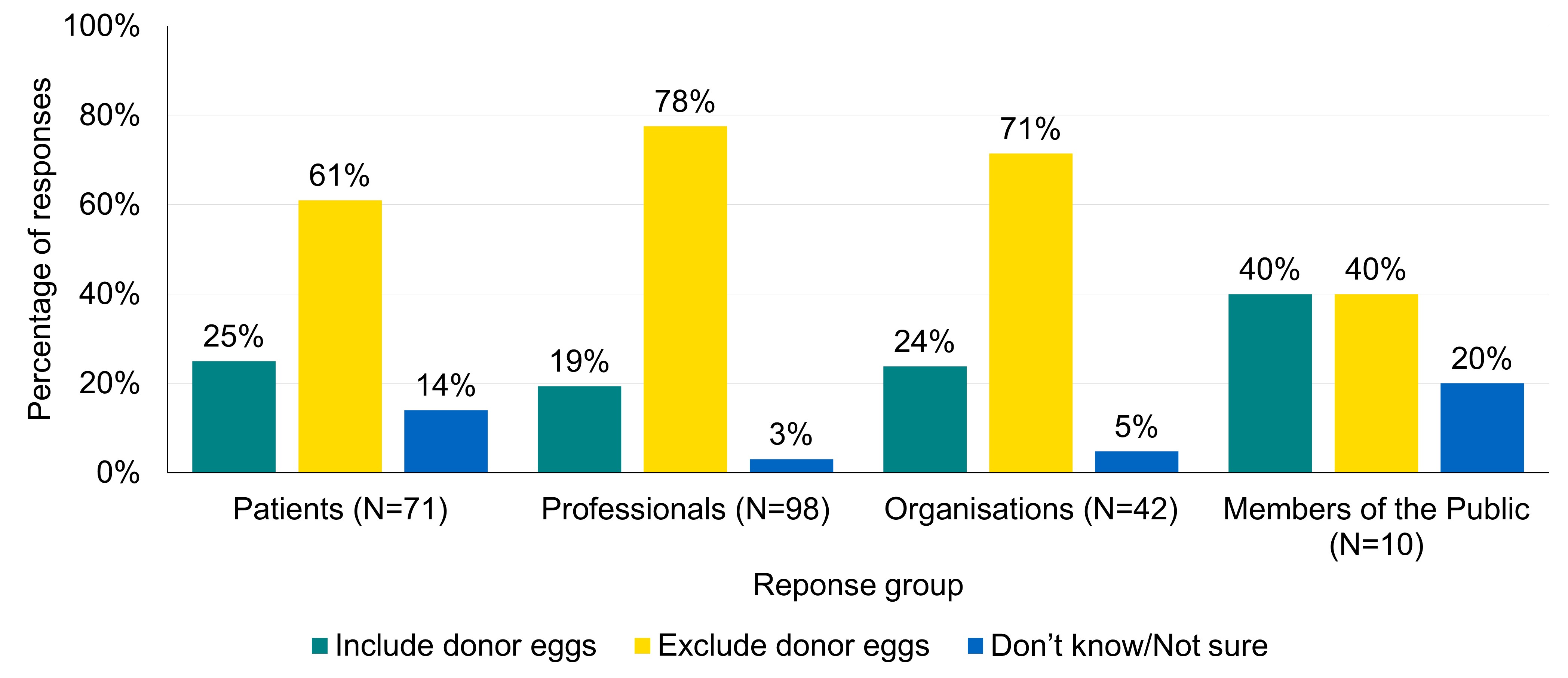
Q: Should treatments using donor eggs be included or excluded from a clinic’s main profile page statistics? Percentages are calculated on the total number of respondents to the question, rather than total respondents to consultation overall. Respondents who answered yes to presenting the profile page statistic as a combined rate were excluded from this question (N=44). A total of four professionals and one organisation skipped this question (N=221).
Download the underlying data for Figure 8 as Excel Worksheet
Responses from organisations and professionals on excluding donor eggs in the main clinic profile statistic commonly stated that, in their view, combining patient and donor eggs could be misleading to patients. This was due to the impact of patient age on fertility and its subsequent effect on outcomes of treatment. A few respondents clarified that they wanted to see outcomes from donor eggs reported on, but separately.
A small number of patients provided free text responses highlighting their views on the inclusion/exclusion of donor eggs. Most felt these should be separated out as they are “distinctive” and would make it “nearly impossible” to choose a clinic. However, there were comments from patients who felt that, while it was important to separate these out, it would not be appropriate to exclude these cycles from statistics overall.
“To mix egg donation statistics would change the data completely as it might indicate a clinics success treating a 43-year-old but it makes a huge difference if they are not her eggs. Transparency is key”
-A prospective, current or past fertility patient sharing personal views.
Pre-implantation genetic testing for aneuploidy (PGT-A)
Respondents were asked whether treatments with PGT-A should be included or excluded from a clinic’s main profile page statistic.
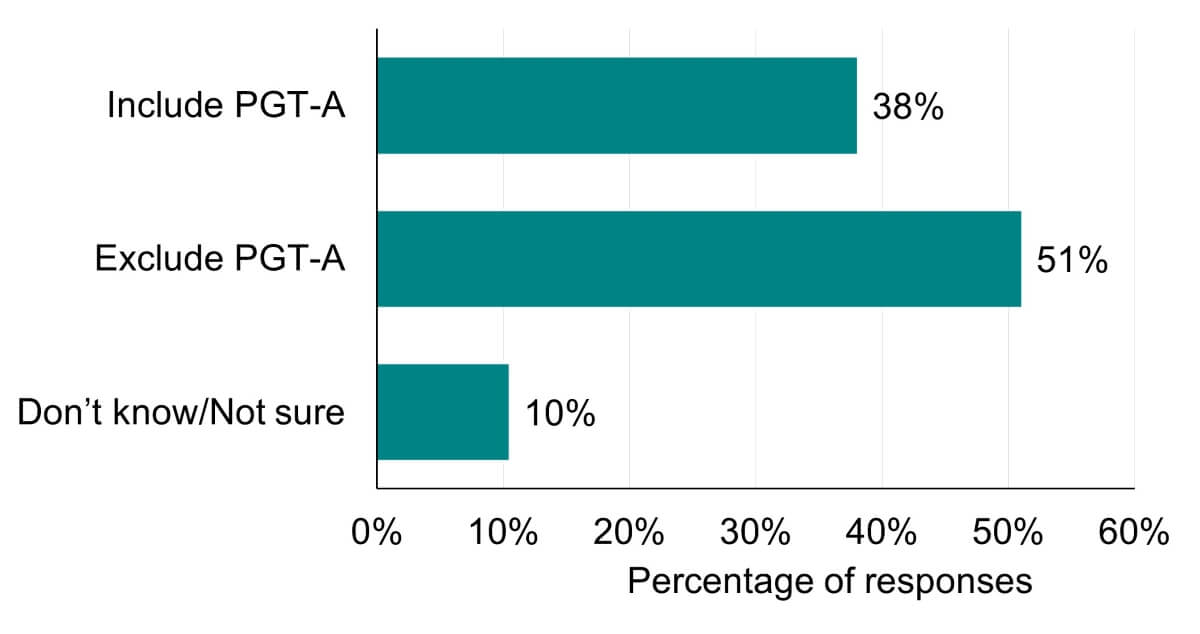
Half (51%) of respondents were in favour of treatments using PGT-A being excluded from a clinic’s main profile page statistic. However, 38% were in favour of including treatments using PGT-A in a clinic’s main profile page statistic (Figure 9).
Differences were seen between response groups (Figure 10). Patients’ views were mixed, with a slight preference for including PGT-A in a clinic’s main profile page statistic (42% vs 38% exclude treatments using PGT-A). Professionals (59%), organisations (56%) and members of the public (50%) were generally in favour of excluding PGT-A from the profile page statistic. Patients (20%) and members of the public (20%) more commonly reported that they were unsure about whether to include PGT-A treatments.
Figure 9. Views on including treatments using PGT-A in a clinic’s main profile page statistic
Q: Should treatments using PGT-A be included or excluded from a clinic’s main profile page statistics? Percentages in the above figure are calculated on the total number of respondents to the question, rather than total respondents to consultation overall. Respondents who answered that yes to presenting the profile page statistic as a combined rate were excluded from this question (N=44). A total of five respondents skipped this question (N=221).
Download the underlying data for Figure 9 as Excel Worksheet
Figure 10. Views on including treatments using PGT-A in a clinic’s main profile page statistic by response group
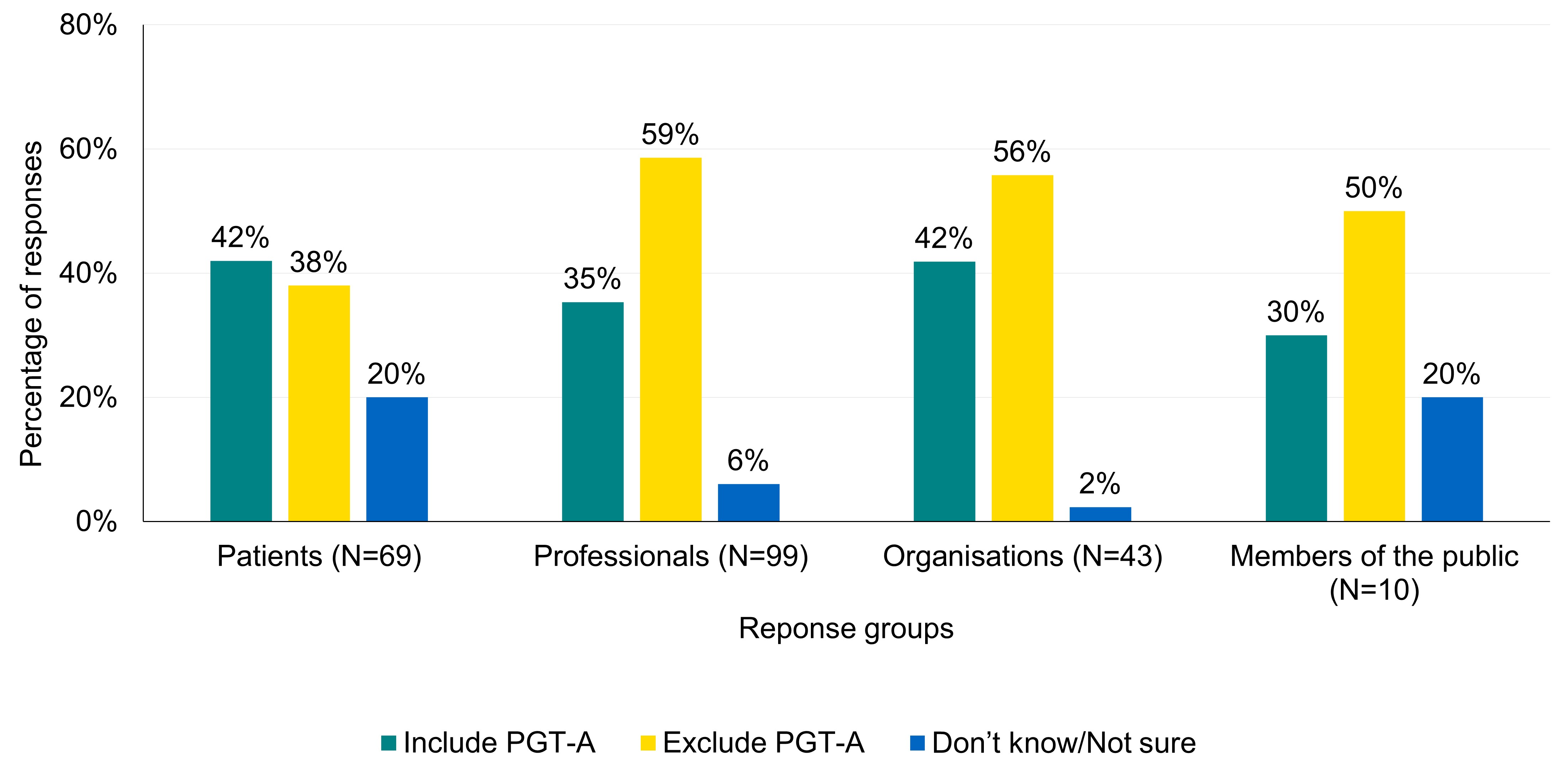
Q: Should treatments using PGT-A be included or excluded from a clinic’s main profile page statistics? Percentages are calculated on the total number of respondents to the question, rather than total respondents to consultation overall. Respondents who answered that yes to presenting the profile page statistic as a combined rate were excluded from this question (N=44). A total of two patients and three professionals skipped this question (N=221).
Download the underlying data for Figure 10 as Excel Worksheet
Patients who mentioned PGT-A in their responses wanted the outcomes PGT-A displayed separately, to not “confuse statistics”. Most responses from professionals and organisations also stated that outcomes of PGT-A should be reported separately for the same reasons. Some responses from professionals and organisations voiced concerns that including treatments using PGT-A may mislead patients about the “actual effect of PGT-A”. References were made to the HFEA’s treatment add-ons list, which states PGT-A has limited evidence of increasing the chance of having a baby for most patients.
“Presentation on Choose a Clinic website: The way PGT-A is presented should be carefully considered, to avoid creating the impression of endorsement of a technique currently rated red for its effectiveness in increasing success rates.”
-An individual sharing their professional views.
A small number of responses from organisations/professionals were in favour of including PGT-A in a clinic’s main profile page statistic.
Additional considerations for the HFEA
Many of the responses highlighted additional considerations for the HFEA to take into account around presenting data on CaFC. These mainly included ways to increase clarity and transparency for patients and the public.
Several suggestions were made for additional information to be included such as more demographic breakdowns or links to additional verified data sources. Many of the suggested additional statistics mentioned, such as number of egg collections or embryo transfers and outcomes by treatment type, are already available in the “View detailed statistics” section of CaFC (see Authority paper). Suggestions were also provided on how additional tools, such as visual aids and plain language, could be used.
Many comments outlined future developments they would like to see to the CaFC tool to make it easier for patients and the public to find reliable information about HFEA-licensed clinics. While outside the scope of this consultation, these responses will form part of future work undertaken by the HFEA to review how information on clinics and the outcomes of treatments are presented.
About the HFEA
The HFEA is the UK’s independent regulator of fertility treatment and research using human embryos. Set up in 1990 by the Human Fertilisation and Embryology Act, the HFEA is responsible for licensing, monitoring, and inspecting fertility clinics and research centres – and taking enforcement action where necessary – to ensure everyone accessing fertility treatment receives high quality care.
The HFEA is an ‘arm’s length body’ of the Department of Health and Social Care, working independently from Government providing free, clear, and impartial information about fertility treatment, clinics and egg, sperm, and embryo donation.
The HFEA collects and verifies data on all treatments that take place in UK licensed clinics, which can support scientific developments and research and service planning and delivery.
The HFEA is funded by licence fees, IVF treatment fees and a small grant from UK central government. For more information, visit hfea.gov.uk.
Contact us regarding this publication
Media: press.office@hfea.gov.uk
Statistical: intelligenceteam@hfea.gov.uk
| Publication date: |
|---|