
Download the underlying dataset as Excel Worksheet.
Table of contents
- Main points
- Foreword
- HFEA regulatory response to the COVID-19 pandemic
- 1. NHS-funded IVF treatment slower to recover
- 2. Treatments decreased by 20% from 2019 to 2020
- 3. Greater decrease in IVF cycles among younger patients and patients in heterosexual relationships
- 4. Egg donor registrations decreased by 23% from 2019 to 2020
- 5. Impact of COVID-19 varied by nation and English region
- 6. COVID-19 caused delays in GP appointments and fertility treatment
- 7. Patient described experiences in COVID-19 related changes to service
- About our data
Main points
- Fertility treatments were suspended across the UK on 15 April 2020, along with other elective medical treatments, due to the impact of COVID-19 on the National Health Service (NHS).
- We set out a framework governing the resumption of treatment during the ongoing pandemic. Clinics could apply to reopen from 11 May 2020 by submitting a self-assessment outlining their strategy on how a safe service could be delivered for patients and staff.
- Private fertility clinics reopened faster than NHS clinics, with 83% of private and 34% of NHS clinics approved to resume service by 15 May, although it should be noted that many private clinics also treat NHS patients. By November 2020, nearly all private and NHS clinics had approvals to reopen.
- NHS-funded IVF treatments decreased across the UK from 35% in 2019 to 28% in 2020.
- Privately funded IVF cycles exceeded 2019 levels in July 2020, whereas NHS-funded IVF cycles had yet to reach 2019 levels by June 2021.
- IVF treatments using fresh embryos decreased by 28% from 2019 to 2020, compared to an 11% decrease in frozen embryo transfer IVF.
- Embryo storage increased by 6% from 2019 to 2020 and was the only activity to increase from 2019 to 2020.
- IVF cycles decreased by 25% among patients aged 18-34 from 2019 to 2020, compared to a 15% decrease among patients aged 40-50. This shows that clinics followed professional body guidance on prioritising patient groups.
- Patients in heterosexual relationships had a 22% decrease in IVF cycles from 2019 to 2020 compared to a 6% decrease among patients in female same-sex relationships.
- Registrations for new egg donors decreased by 23% from 2019 to 2020, compared to an 14% decrease in new sperm donor registrations.
- The decreases in IVF cycles varied across the four nations, with a 39% decrease in IVF cycles in Wales from 2019 to 2020 compared to a 19% decrease in England.
- In our recent national patient survey, 10% of patients having treatment from 2020-2021 said that COVID-19 caused a delay in speaking with a GP, and 28% said that COVID-19 caused a delay to starting treatment.
- Black, Asian, Mixed or Other ethnicity patients were more likely to have reported a delay in speaking with a GP due to COVID-19 (20%) compared to White patients (9%).
- Survey respondents were twice as likely to report a delay to starting treatment due to COVID-19 if they were NHS-funded (41%) compared to privately funded (21%).
- Patients mentioned concerns over restrictions in partner attendance to clinic appointments due to COVID-19, NHS waiting lists and the use of online/phone appointments in open-text responses to our survey.
Foreword
Maintaining an effective fertility service throughout the COVID-19 pandemic has required commitment and hard work from fertility clinic staff across the UK. All staff will have had to cope with staff shortages due to absence and some will have experienced personal bereavements. Throughout the pandemic, staff were challenged to provide a safe service for patients, while dealing with the pressures of national restrictions in their professional and personal lives.
This report notes the impact on patients following the short closure of clinics during the UK’s first national lockdown in Spring 2020 and where, on re-opening, clinics prioritised existing and older patients in line with professional guidance. Our data shows what was expected with fewer treatments among younger patients, and a decrease in other treatments, for example new egg donors.
We note that a range of NHS women’s services experienced delays due to COVID-19. Despite being the first elective health service to re-open in the first stages of the pandemic, the fertility sector has not been immune to these pressures. The knock-on effect of delays across healthcare, especially gynaecological services where tests or surgery may be needed before starting fertility treatment, has meant that some patients will be experiencing delays in accessing fertility services.
Most HFEA licensed clinics, whether private or NHS, treat both NHS and privately funded patients. However, NHS clinics were slower to open than clinics in the private sector in 2020. This may be because more NHS staff were redeployed to work in other areas of hospital services and the reduction in non-emergency patients entering a hospital environment. Additionally, private clinics may have re-commenced services at a faster rate because of the pressures on their finances. As a result, NHS treatment numbers decreased most in 2020, though they have not dropped by as much as we might have expected as many NHS patients are treated in private units.
Patients also experienced changes in how their treatment was carried out during the pandemic, for example, the increased use of phone/video appointments and restrictions in partners attending appointments. While some patients reported their distress with these changes in our recent national patient survey, it is important not to lose sight of the extraordinary efforts made by clinic staff to reopen safely and stay open through subsequent lockdowns and restrictions.
This report summarises the impact of COVID-19 on fertility treatment in the UK. The data shown is a snapshot of what happened at a particular time (2020), and we do not underestimate the possible long-term impact of working in a clinic or being a patient during the pandemic.
HFEA regulatory response to the COVID-19 pandemic
The NHS was placed under unprecedented strain during the first wave of the COVID-19 pandemic in Spring 2020 when measures were put in place by the Westminster and devolved governments to restrict movement in national lockdowns. In response to those national restrictions, the suspension of NHS elective surgery and UK professional body guidance, we made the difficult decision on 23 March 2020 to require all clinics to cease fertility treatments by 15 April 20201.
Non-elective fertility preservation was the only treatment permitted throughout the suspension (for example, patients storing their eggs or sperm who were about to start chemotherapy). Many clinics were reduced to minimal staffing levels, with staff redeployed to work in hospitals or furloughed.
As new professional body guidance2 was developed which set out how clinics could offer safe services, we put in place a regulatory framework governing the resumption of treatment during the ongoing pandemic. From 11 May 2020, clinics could apply to the HFEA for permission to reopen by submitting a self-assessment questionnaire which outlined their treatment commencement strategy3,4. The strategy set out how a safe service could be delivered to patients and staff. Clinic strategies typically included a range of measures to reduce clinic occupancy, including the use of video/phone appointments and restrictions on partners from attending all non-essential appointments.
Many clinics were able to restart treatments quickly, adapting and introducing new ways of delivering safe services. This meant that the UK fertility sector was the first elective medical sector to reopen during the pandemic.
By the end of the first week that clinics could apply to reopen (week starting 11 May 2020), 83% of private clinics and 34% of NHS clinics had received approval from the HFEA. By the end of October 2020, 97% of private and 95% of NHS clinics had approval to reopen5.
The detailed plans that clinics had to put in place to ensure patients could be treated safely, has meant they have been able to continue to offer treatment during all subsequent lockdowns and restrictions.
1. NHS-funded IVF treatment slower to recover
In response to COVID-19 IVF treatments across the UK were suspended from 15 April to 11 May 2020. NHS-funded IVF treatments saw a larger total decrease of 35% from 2019 to 2020 compared to a 13% decrease in privately funded cycles. It is important to note both NHS and private clinics treat NHS-funded patients.
As clinics were permitted to reopen in May 20203, both NHS and privately funded IVF cycles increased (Figure 1). Privately funded IVF cycles increased at a faster rate than NHS cycles and exceeded 2019 figures in July 2020. In contrast, NHS-funded IVF cycles had yet to reach 2019 levels by June 2021, with the exception of December 2020. It should be noted that NHS-funded cycles can be carried out in private clinics and vice versa. See section 5 for funding information by nation and region.
The decrease in NHS-funded IVF cycles can be explained in part by the greater impact of the pandemic on the NHS as a whole, and the slower return of NHS clinics following treatment suspensions (see introduction). In addition, many patients require further investigations or surgeries within the NHS where they may be experiencing higher waiting times before being able to access NHS-funded treatment or start privately funded treatment6.
Figure 1. NHS-funded IVF cycles decreased following COVID-19 outbreak
Number of IVF cycles by month and funding, January 2019-June 2021
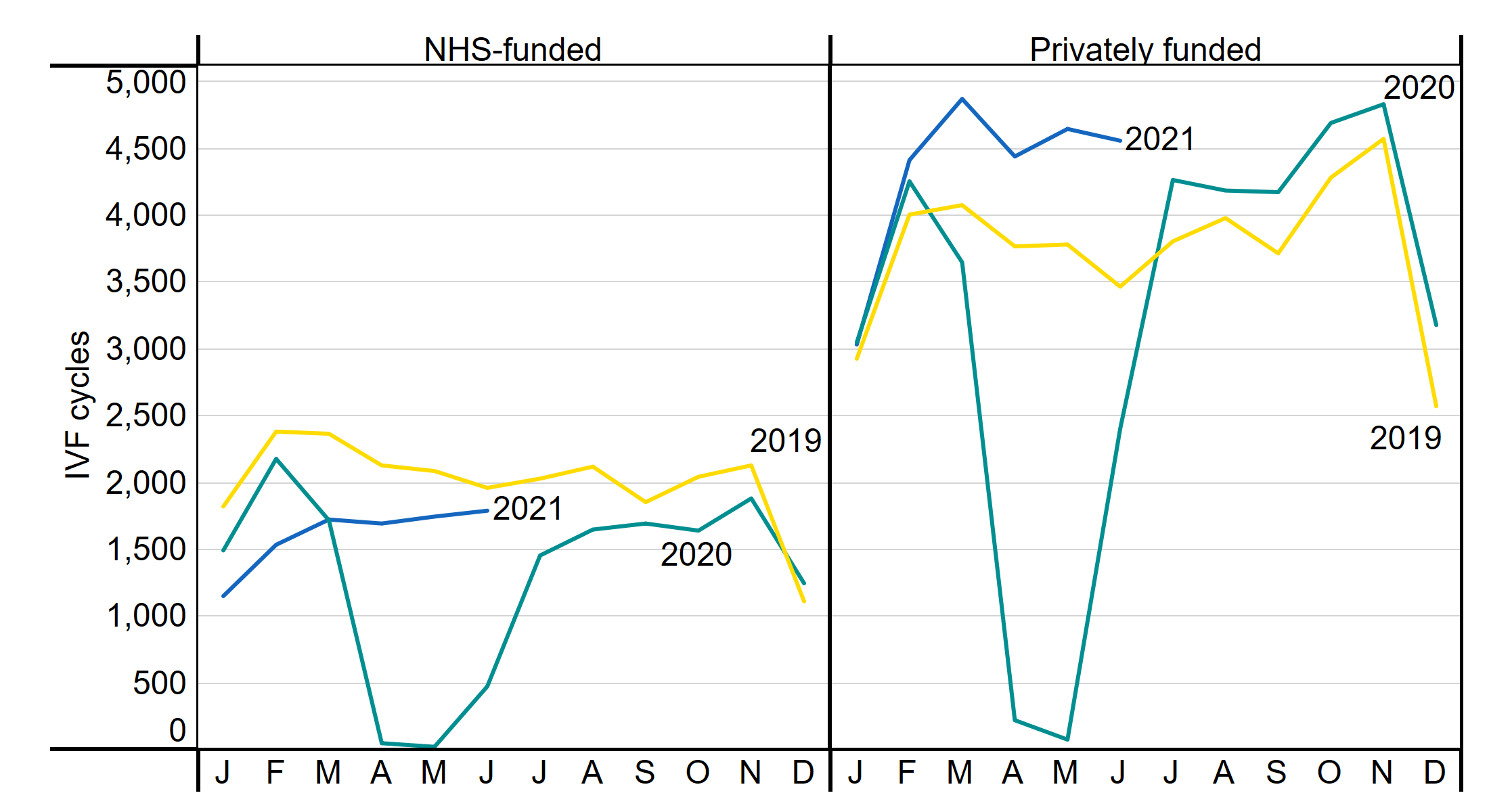
Note figure 1: This data includes treatment cycles and IVF only.
Download the underlying data for Figure 1 as Excel Worksheet.
2. Treatments decreased by 20% from 2019 to 2020
Nearly 60,000 cycles of fertility treatment took place during the ongoing pandemic in 2020. However, IVF and DI treatments decreased overall by 20% from 2019 to 2020, which was mainly caused by a 28% decrease in fresh embryo transfer IVF cycles during that period (Table 1). DI cycles decreased by 10% and frozen embryo transfer IVF cycles by 11% from 2019 to 2020. Frozen embryo transfer IVF has been increasing in use in the UK, accounting for 27% of all IVF cycles in 2015 and 46% in 2020.
Embryo storage cycles were the only activity that increased from 2019 to 2020 (+6%). Embryo storage is the fastest growing activity in recent years, having increased by 13% from 2018 to 2019 (see Fertility Trends 2019).
The smaller impact on embryo storage cycles may relate to the guidance for clinics to take a more cautious approach during the pandemic to patients at higher risk of developing ovarian hyperstimulation syndrome (OHSS), as patients who develop OHSS can require hospitalisation. Clinics were advised to use elective freeze all, which reduces OHSS risk, for patients at greater risk of developing OHSS2,7. Additionally, patients may have chosen to store their embryos rather than receiving embryo transfers due to concerns around COVID-19.
Donation cycles decreased by 23% from 2019 to 2020. Egg share cycles saw the largest decrease of 37%, though from a small base, falling from 300 cycles in 2019 to 190 in 2020. See section 4 for further information on donation.
Table 1. The number of treatment cycles decreased by 20% from 2019 to 2020
Number of cycles by intended activity, 2019 and 2020
| 2019 | 2020 | % change | |
| DI | 5,706 | 5,115 | -10% |
| IVF - fresh embryo transfer | 40,712 | 29,352 | -28% |
| IVF - frozen embryo transfer | 28,347 | 25,200 | -11% |
| Treatment total | 74,765 | 59,667 | -20% |
| Egg storage | 2,397 | 2,267 | -5% |
| Embryo storage | 8,228 | 8,731 | +6% |
| Storage total | 10,625 | 10,998 | +4% |
| Donation | 2,018 | 1,548 | -23% |
| Egg share | 300 | 190 | -37% |
| Donation total | 2,318 | 1,738 | -25% |
Note table 1: IVF and DI data include only treatment now.
Download the underlying data for Table 1 as Excel Worksheet.
3. Greater decrease in IVF cycles among younger patients and patients in heterosexual relationships
The average age for patients having IVF treatment was 36 in 2019, with around 40% of IVF treatments among patients 18-34 years of age. Following COVID-19, the number of IVF cycles decreased for all ages from 2019 to 2020, with the largest decrease among patients aged 18-34 (-25%). In contrast, patients aged 40-50 had a 15% decrease in IVF cycles from 2019 to 2020. The smaller decrease among older patients is in line with professional guidance recommending clinics prioritise older patients following service suspension, as the chance of having a live birth following fertility treatment decreases with age7,8.
When comparing by funding and age, there was a larger decrease in younger patients having NHS-funded cycles than privately funded patients (Figure 2). There was a 38% decrease in the number of NHS-funded IVF cycles for patients aged 18-34 from 2019 to 2020, compared to a 13% decrease among privately funded patients aged 18-34.
In response to our National Patient Survey 2021, some patients wrote about experiencing long waiting times to access NHS treatment due to COVID-19. The increased use of privately funded treatment may relate to patients opting to go private rather than waiting for access to NHS services. See section 7 for further information on responses to our survey.
Figure 2. NHS patients under 35 were more impacted than their privately funded patients
Number of IVF cycles by funding type and patient age group, 2016-2020
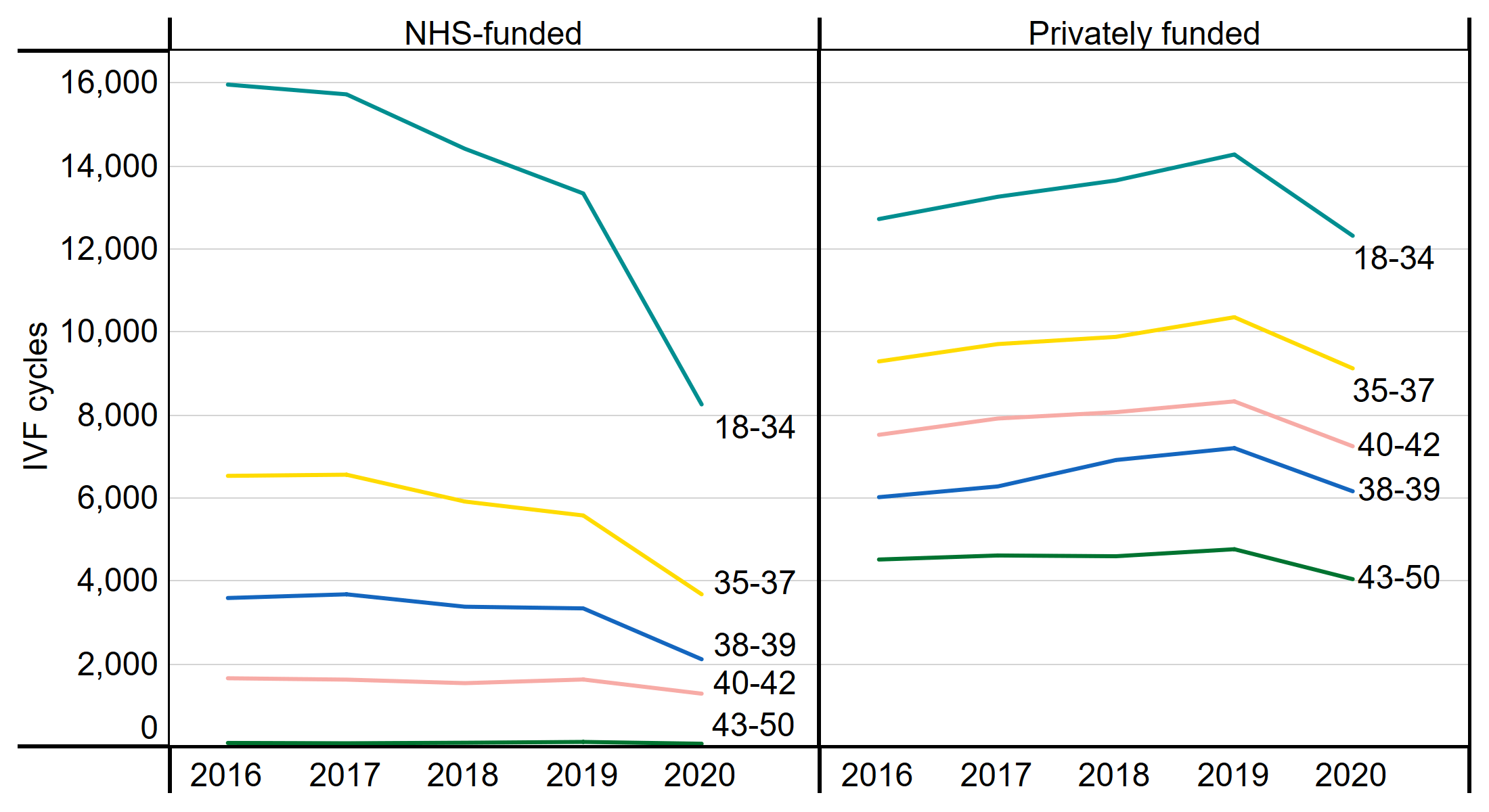
Note figure 2: This data includes treatment cycles and IVF only. Where no age is indicated cycles have been excluded.
Download the underlying data for Figure 2 as Excel Worksheet.
Around 94% of patients using IVF treatment were in heterosexual relationships, followed by patients in female same-sex relationships (4%), single patients (2%) and surrogates (0.5%) from 2018-2020. Patients in heterosexual relationships experienced a greater impact from COVID-19 with a 22% decrease in IVF cycles from 2019 to 2020 (Table 2). In comparison, patients in female same-sex relationships had a 6% decrease in IVF cycles.
In 2018-2019 most DI treatments were among patients in female same-sex relationships (45%) or single patients (18%), followed by patients in heterosexual relationships (36%). Patients in heterosexual relationships had a 17% decrease in DI cycles from 2019 to 2020, compared to a 9% decrease among patients in female same-sex relationships (Table 2).
In 2018, we reported that 39% of IVF cycles among patients in heterosexual relationships were funded through the NHS compared to 14% among patients in female same-sex relationships9. As NHS-funded cycles were most impacted following COVID-19, this may in part explain the larger decrease in cycles among heterosexual couples.
Younger patients, particularly those in heterosexual relationships, may also have postponed treatment due to delays in accessing funding or reticence to have fertility treatment or a pregnancy during the pandemic. Indeed, a UK survey of 504 women planning a pregnancy showed that 38% had decided to postpone due to COVID-1910.
Table 2. Patients in heterosexual relationships had largest decreases in IVF and DI treatments from 2019 to 2020
Number of IVF and DI cycles by partner, 2019 and 2020
| 2019 | 2020 | % change | ||
| IVF | Male partner | 64,849 | 50,608 | -22% |
| Female partner | 2,440 | 2,305 | -6% | |
| No partner | 1,473 | 1,407 | -4% | |
| Surrogate | 326 | 266 | -18% | |
| DI | Male partner | 2,127 | 1,773 | -17% |
| Female partner | 2,549 | 2,332 | -9% | |
| No partner | 1,030 | 1,010 | -2% | |
Note table 2: This data includes treatment cycles.
Download the underlying data for Table 2 as Excel Worksheet.
4. Egg donor registrations decreased by 23% from 2019 to 2020
The use of egg and sperm donation in treatment increased from 2019 to 2020, accounting for 21% of treatments (IVF and DI) in 2019 and 23% of treatments in 2020. However, donor registrations decreased during this period. New egg donor registrations decreased by 23% from 2019 to 2020, whereas sperm donors decreased by 14% (Figure 3).
The decrease in new donor registrations may relate to local lockdowns and hesitancy from potential donors around COVID-19 safety. Additionally, when re-starting treatment in May 2020, clinics prioritised patients who had experienced delays to treatment on resuming services rather than seeking new donations.
Figure 3. Egg donor registrations decreased 23% from 2019 to 2020
Number of new egg and sperm donor registrations, 2016-2020
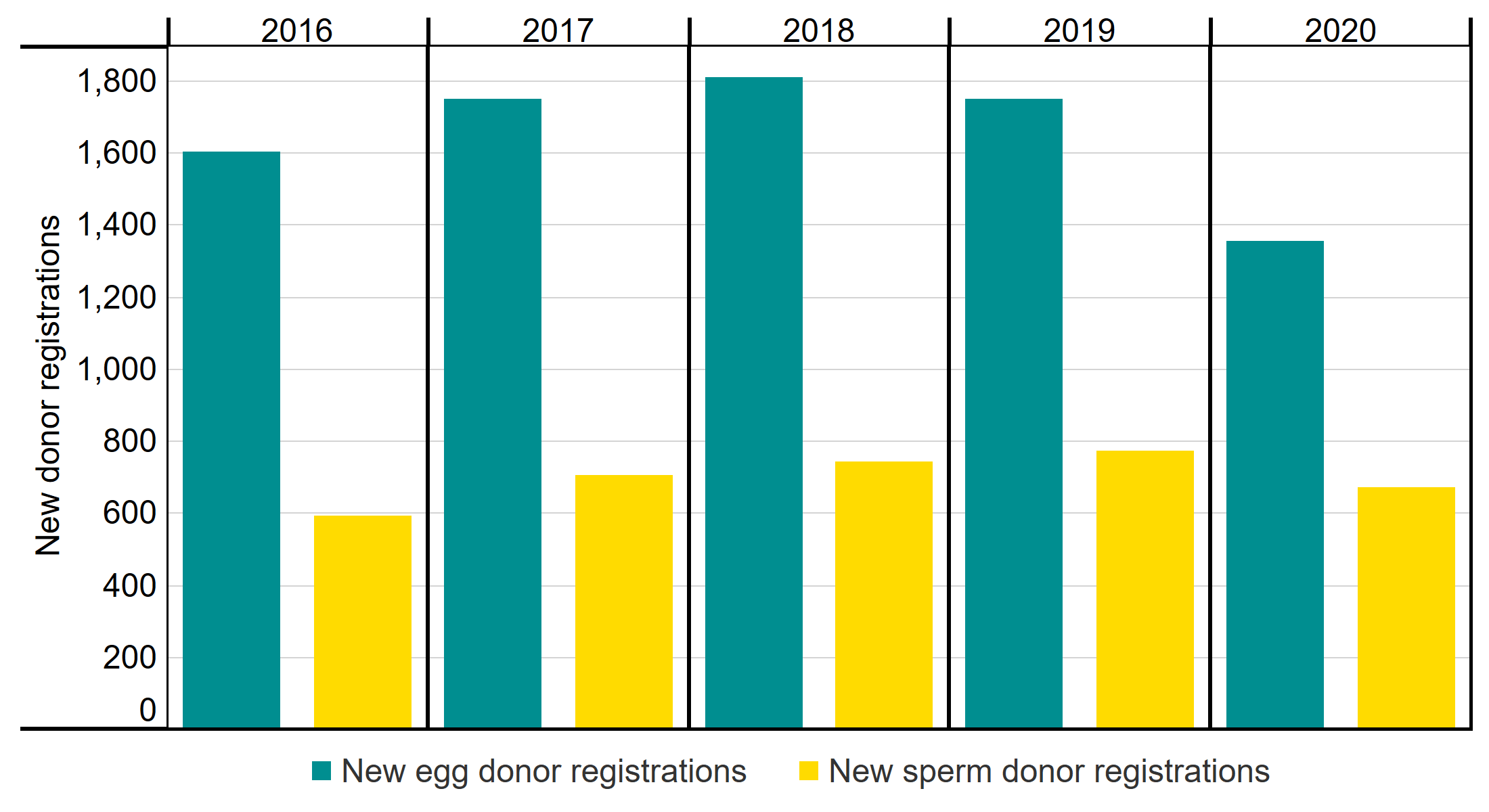
Note figure 3: This data uses new egg and sperm donor registrations only. Donors that registered multiple times will only be counted in the year of their first registration.
Download the underlying data for Figure 3 as Excel Worksheet.
5. Impact of COVID-19 varied by nation and English region
The impact of COVID-19 on IVF treatments between 2019 and 2020 varied across the UK (Table 3). The largest decreases in IVF treatment by nation were seen in Wales (-39%), followed by Scotland (-27%). IVF cycles in England reduced by the least of any nation (-19%). Northern Ireland’s largest clinic had data reporting issues that meant we were unable to report 2020 values for comparison.
These differences likely relate to local restrictions and the speed at which individual clinics reopened. The smaller decrease in cycles in England compared to other nations is likely explained by the higher proportion of private funding used in England, as NHS-funded cycles were most impacted in 2020 (see section 1 and Table 4). NHS-funded treatments are commonly carried out at private clinics and vice versa.
Table 3. Impact of COVID-19 varied by nation and English region
Number of IVF cycles by nation and English region, 2019 and 2020
| 2019 | 2020 | % change | |
| *Northern Ireland | 1,429 | N/A | N/A |
| Scotland | 4,765 | 3,466 | -27% |
| Wales | 2,771 | 1,696 | -39% |
| England | 60,125 | 48,754 | -19% |
| East Midlands | 3,830 | 3,276 | -14% |
| East of England | 3,921 | 3,148 | -20% |
| London | 22,027 | 17,977 | -18% |
| North East | 2,279 | 1,560 | -32% |
| North West | 8,571 | 7,028 | -18% |
| South East | 7,609 | 6,548 | -14% |
| South West | 3,412 | 2,846 | -17% |
| West Midlands | 4,559 | 3,235 | -29% |
| Yorkshire and the Humber | 3,917 | 3,136 | -20% |
Note table 3: This data includes treatment cycles and IVF only.
*Data for Northern Ireland has been excluded for 2020 due to data reporting issues at one clinic accounting for about 1,200 cycles (83% of annual cycles in Northern Ireland).
Download the underlying data for Table 3 as Excel Worksheet.
Most IVF cycles in the UK are funded privately. From 2009-2017 around 40% of IVF cycles were funded through the NHS, with decreases in the last few years to 35% in 2019 and 28% in 2020 (Table 4).
The number of NHS-funded IVF cycles decreased across all four nations with the largest decrease in Wales from 39% NHS-funded in 2019 to 30% in 2020. In England, NHS-funded IVF cycles decreased from 32% in 2019 to 26% in 2020, and in Scotland, NHS-funded IVF cycles decreased from 62% to 59%. As noted earlier, Northern Ireland data was not available in 2020 due to data reporting issues at their largest centre.
The decrease in NHS-funded IVF cycles in all four nations is likely not due to changes in available funding, but due to difficulty in accessing treatments such as clinic closures or delays in accessing tests or surgeries prior to starting treatment.
Table 4. NHS-funded IVF cycles decreased across all nations and most English regions
Proportion of IVF cycles funded by the NHS by nation and English region, 2019 and 2020
| 2019 | 2020 | |
| *Northern Ireland | 38% | N/A |
| Scotland | 62% | 59% |
| Wales | 39% | 30% |
| England | 32% | 26% |
| East Midlands | 38% | 36% |
| East of England | 20% | 17% |
| London | 23% | 14% |
| North East | 56% | 54% |
| North West | 53% | 46% |
| South East | 31% | 26% |
| South West | 39% | 29% |
| West Midlands | 40% | 32% |
| Yorkshire and the Humber | 26% | 31% |
| UK total | 35% | 28% |
Note table 4: This data includes treatment cycles and IVF only.
*Data for Northern Ireland has been excluded for 2020 due to data reporting issues at one clinic accounting for about 1,200 cycles (83% of annual cycles in Northern Ireland).
Download the underlying data for Table 4 as Excel Worksheet.
6. COVID-19 caused delays in GP appointments and fertility treatment
We carried out a National Patient Survey at the end of 2021, open to anyone who had fertility treatment within the last ten years, to assess user experience in receiving fertility treatment at UK clinics.
In survey questions evaluating delays in speaking with a GP or starting treatment, COVID-19 was included as an option. To understand the impact of COVID-19 more accurately, we only evaluated survey data from patients who had treatment in 2020 or 2021.
6.1. Delays in speaking with a GP
Patients were asked to select reasons for their wait to speak to a GP about their treatment options. One in ten patients (10%) having treatment in 2020/2021 said that COVID-19 caused a delay in speaking with their GP before starting treatment (N=502).
When comparing differences by ethnicity, patients of ethnic minority groups were more likely to have reported COVID-19 as a cause for their delays in speaking to a GP. One in five Black, Asian, Mixed or Other ethnicity patients reported a delay in speaking with a GP due to COVID-19 (20%, N=64) compared to one in ten White patients (9%, N=437). In reasons for a delay in speaking with a GP, patients from Black, Asian, Mixed or Other ethnic groups more commonly stated a difficulty in accessing appointments (14%, N=64) compared to White patients (9%, N=437)11.
Patients of all ages reported similar delays in speaking with a GP due to COVID-19, indicating that the greater impact of COVID-19 on younger age groups (see section 2) was likely not a result of access to GP appointments.
We should note that these are self-reported delays, so we cannot assess whether patients delayed accessing their GP because they felt the GP was prioritising managing the pandemic, or whether the patient tried to access their GP to discuss treatment and was told there would be a delay or postponed appointment because of COVID-19.
6.2. Delays in starting treatment
Survey respondents were asked to select reasons for any delays in starting treatment after speaking to a GP. Over a quarter of patients (28%) who had treatment in 2020/2021 said that COVID-19 caused a delay in starting fertility treatment (N=710). Most patients who had experienced delays in starting treatment due to COVID-19 had also experienced delays in accessing further tests or surgeries and/or NHS waiting lists (66%, N=201). These experiences match with findings from the Royal College of Obstetricians and Gynaecologists report which found that gynaecology waiting lists have faced the biggest increase as a result of the pandemic of all medical specialities6.
The widest variation in delays to starting treatment was by funding type. NHS-funded patients were twice as likely (41%, N=263) to have experienced a delay to starting treatment due to COVID-19 compared to privately funded patients (23%, N=277). See section 1 for more information on funding.
There was no difference in delays to starting treatment due to COVID-19 by patient ethnic group. This is supported by HFEA register data which showed Black, Asian, Mixed or Other ethnicity patients and White patients had similar decreases in their number of IVF cycles from 2019 to 2020 (see underlying data).
Almost a third of patients 18-34 years of age reported a delay to starting treatment due to COVID-19 (31%, N=322) compared to one in five patients aged 40+ (20%, N=99)11. See section 2 for more information on how COVID-19 impacted patients by age.
Patients with male partners were more likely to have experienced delays in starting their treatment due to COVID-19 (29%, N=619) when compared to patients in female same-sex relationships and single patients (22%, N=90). This may relate to delays in accessing funding for treatment due to COVID-19, as funding is more common among heterosexual couples (see Family formations in fertility treatment 2018).
7. Patient described experiences in COVID-19 related changes to service
Though the fertility sector was the first elective health service to restart after the first lockdown, many patients reported difficulties in service changes due to COVID-19. Patients responding to our National Patient Survey 2021 mentioned COVID-19 and its impact on their treatment in open-text responses. Patients wrote about how certain clinic policy changes, which enabled clinics to restart services quickly and reduce risk of COVID-19 infection, negatively affected their experience. Additionally, some patients wrote about experiencing delays in accessing NHS services. However, it is also important to note that many responses mentioned positive experiences with clinic staff and showed an understanding of the strain many healthcare workers were under due to COVID-19.
Many patients mentioned difficulties in not having their partner present for all appointments due to clinic COVID-19 measures. These policies were commonly used in clinic strategies to continue treatment in a COVID-19 secure manner by reducing occupancy in the clinic where possible. Patients missed the emotional support that their partner could offer them during appointments and procedures. They also felt added responsibility when having to make decisions without their partner present and having to relay important information to their partners.
“…my wife couldn't be with me for much of my treatment. The clinic did all they could to make sure we were both supported though, and despite some emergencies, traumas and failed cycles we have felt respected and supported by [our clinic]…”
“I’ve never felt so alone in the whole process as I do now…Having to relay important information to my husband about our embryos, why is this being discussed with me alone? They are both of ours.”
“… my husband wasn't allowed into the clinic for the majority of the treatment, [but] the clinic were extra supportive during appointments…”
“… My partner was not allowed to attend any treatment or scan appointments which was very upsetting, but I do understand the circumstances.”
“…I had to attend all scans, tests, egg collection and transfer on my own. This was hard for me but also difficult for him to feel involved and hear all the information.”
Some patients described struggles relating to the move to online and over the phone appointments. Patients felt that they did not receive the same level of care that they may have received if appointments had been in person. Some patients also described difficulties in accessing appointments and getting in contact with both clinics and GPs during the pandemic. As noted earlier, during the first lockdown, when treatment was suspended from mid-April to mid-May, many clinic staff were redeployed to work in hospitals or furloughed. With the shift to online/phone appointments, some clinics have experienced increases in uptake of counselling. They have mentioned patients/partners being more easily able to balance schedules and feeling more at ease in the familiarity of their own home.
“…it was done over the phone which I didn’t feel helped me from a mental well-being perspective.”
“They told me they were too busy with COVID to help.”
“…the majority of the staff were kind and helpful - they were just rushed off their feet.”
“It all felt very impersonal but appreciate that there was a pandemic and it was a difficult situation which couldn’t be helped…”
Difficulty in accessing NHS services was also mentioned in some open-text responses to the survey. Patients described feeling put off by long waiting lists and considering using private funding to access treatment faster. A recent report found that gynaecological services wait times in the UK increased by 60% following COVID-196. These delays will have affected many patients requiring further tests or surgeries before starting fertility treatment.
“My GP was really helpful and immediately referred us for the initial tests but due to covid a lot of these were delayed.”
“We now have a beautiful baby boy, but if we waited with the NHS he wouldn’t be here now.”
“My second cycle which is NHS funded, should have had an appointment within 1-2 months, I am still waiting 2 months later.”
“I was very disappointed with the NHS treatment, felt I kept being put off for long periods before even making it to waiting lists…ended up having to go private to get things moving.”
Some patients also mentioned positive experiences with clinic staff, mentioning the work of staff to make them feel more comfortable during procedures where possible. Additionally, some patients wrote about clinics adapting to individual patient needs, such as accelerating treatments for those with cancer diagnoses.
“…the nurse showed great compassion for me and allowed my husband to come in too - just during the scan. This meant the world to me. Luckily it was good news!”
“We had already been through fertility testing…and were waiting to start IVF…when I was diagnosed with breast cancer. As soon as we told the clinic, they accelerated us and adapted the schedule around my treatment plan.”
“The hospital we had and continue to have treatment at have been absolutely amazing.”
…[we] were being treated with dignity, respect and empathetic to the situation.”
About our data
Register data
This report largely focuses on 2020/21, although it draws on some data from 2016-2021. Data for 2021 covers a partial year, ending in June 2021. The information that we publish is a snapshot of data provided to us by licensed clinics. The figures supplied in this report are from our data warehouse containing Register data as at 28/08/2021. We have excluded approximately 2,400 cycles due to technical issues at one centre in England that resulted in reporting errors. Additionally, data on Northern Ireland is excluded throughout the report when comparing information by nation, this is due to one clinic accounting for 83% of annual cycles in Northern Ireland experiencing data reporting errors. Results are published according to the year in which the cycle was started. Due to rounding, some percentages may not add to 100%. It is worth noting that NHS-funded cycles take place in private clinics and vice versa.
This report uses unvalidated treatment data for 2020 and 2021. This is because the HFEA has recently launched a new data submission system for clinics and migrated our fertility treatment and outcomes data to a new database. This data migration has resulted in delays which have prevented the use of 2020/21 outcome data, or the validation of the 2020/21 treatment data. Due to the resultant data quality issues, these statistics cannot be classified as official statistics.
For further information, please see our quality and methodology report and information page in the underlying dataset.
Patient survey data
We received a total of 1,868 responses. Once partial completes and screened-out responses had been removed, a total of 1,233 patient were included in the analysis.
The survey was open to anyone who had undergone fertility treatment in the UK in the past ten years, including patients, partners, intended parents and surrogates. It was live between 2 November - 7 December 2021. As this report focuses on the COVID-19 pandemic, we have only included survey responses where the patient had treatment in 2020/21.
The survey is broadly representative of the fertility patient population, with a few exceptions. More details can be found in the survey quality and methodology report. Due to small numbers, we have had to consider responses from patient of Black, Asian, Mixed and Other ethnicity patients together to draw comparisons by ethnicity.
Throughout the report, where NHS-funded and privately funded patients are referenced, this is generally anyone who has ever had NHS-funded only or privately funded only treatment. The report is based on responses from patients, partners, intended parents and surrogates; however, we refer to survey respondents as patients throughout as this covers 95% of respondents.
Contact us regarding this publication
Media: press.office@hfea.gov.uk
Statistical: intelligenceteam@hfea.gov.uk
Accessibility: comms@hfea.gov.uk
Notes on the Impact of COVID-19 on fertility treatment 2020
- General direction 0014 version 1 by HFEA
- The Association of Reproductive and Clinical Scientists (ARCS) and British Fertility Society (BFS) U.K. best practice guidelines for reintroduction of routine fertility treatments during the COVID-19 pandemic by ARCs and BFS, May 2020
- General direction 0014 version 2 by HFEA
- Coronavirus (COVID-19) - previous updates for professionals by HFEA
- There were two small IUI centres that decided not to re-open or had decided to revoke their licence prior to the pandemic
- Left too long: understanding the scale and impact of gynaecology waiting lists by Royal College of Obstetricians & Gynaecologists
- COVID-19 and fertility treatment - previous updates for professionals by HFEA, November 2020
- Prioritizing IVF treatment in the post-COVID-19 era: a predictive modelling study based on UK national data, Human Reproduction, 2020, 36: 666-675
- Family formations in fertility treatment 2018 by HFEA
- The Impact of the COVID-19 Pandemic on Pregnancy Planning Behaviors, Women’s Health Reports, 2021, 2.1:71-77
- This data is a trend but not significantly different
| Publication date: |
|---|